One would expect that in an era where smartphones are more powerful than our computers were 5 years ago, healthcare providers would have an arsenal of healthcare IT solutions to enhance patient care but also optimize their own work-flow. Shockingly, in 2014 most healthcare IT solutions (such as EHR systems) are incapable of basic functions that we take for granted in other aspects of our digital lives (this is despite the fact that hundreds of millions of dollars have been invested by institutions). We have made information electronic, but continue to work with it as if all we had was an abacus. This is problematic since many providers are now involved in taking care of patients (physicians, nurses, physician assistants, clinical pharmacists, therapists, and trainees), and there is greater turnover of team members due to the shift work nature of inpatient care. Rather than having optimal information available – we have data chaos.
The situation is in stark contrast to my out-of-hospital life. In my Gmail I can (usually) easily find a specific message using a combination of ‘has,’ ‘to,’ ‘from,’ and ‘subject’ statements. Most EHRs on the other hand have me scrolling through consultation and progress notes in size 10 text, stacked one on top of each other, which are about as search-able as a Where’s Waldo scene. As a Hospital Medicine doctor who needs to rapidly assimilate information often in the middle of the night – EHR is my last resort. When I receive an emergent page, I rely on my examination, the patient interview (if they’re able to talk), and then a quick glance at a rudimentary ‘sign out’ document handed to me from the day-team. EHR is neither optimized for mobile in most cases, nor can I find anything I am looking for when I actually need it. This is true irrespective of whether I am working at a rural hospital in Maine with a 10 year old EHR, or at a major academic center with a ‘cutting edge’ EHR.
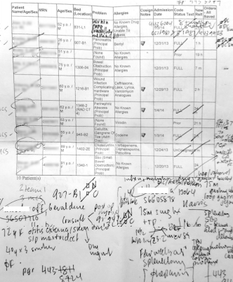
Despite heavy investment in healthcare IT from institutions – providers like myself still find ourselves carrying around printed patient lists with scribbled check boxes and to do lists. The sign out document – a purportedly succinct summary of the patient problems and suggested plan of action quite obviously has pitfalls. One night last week I counted 42 patients I was covering overnight on five different sub-specialty services; and some basic math revealed that in my 12 hour shift I was in charge of more than 120 active medical problems, and at least 1000 years of medical history (conservatively). All of this was summarized for me by other providers in a neatly typed word document extracted from copy-pasted snippets of EHR notes, printed, stapled, and then folded – ready in my white coat pocket for me to peruse while I bolted through corridors or took the elevator to where a patient was crashing.
On discussing the shortfalls of modern healthcare IT solutions; I often hear colleagues stating that change is coming ‘soon’ (read; 2–5 years). Given that medical errors now kill more than 400 000 Americans and are the number three cause of death in the United States – we need a greater sense of urgency about how broken IT systems are, and how we can fix them immediately. Infinitely more thought, investment and energy goes into social networking endeavors than how patient information is presented and made available to healthcare team members. (It is irrefutably easier for me to find out where you went to college – using LinkedIn, Google, or Facebook — than to find out who my patient’s primary care doctor is).
It makes little sense that modern medicine offer us marvels like whole genome sequencing, while simultaneously providing ridiculous solutions such as mnemonics to reduce errors during change of shift. Surely the bar must be set higher, and we must harness the technology we carry in our pockets.
11/4/2014
Varun Verma, M.D. is a board-certified Internal Medicine physician who splits his time as a Hospitalist at Brigham and Women’s Hospital (Boston) and as a Senior Clinical Advisor to Possible (Nepal)
@VarunVermaMD
The situation is in stark contrast to my out-of-hospital life. In my Gmail I can (usually) easily find a specific message using a combination of ‘has,’ ‘to,’ ‘from,’ and ‘subject’ statements. Most EHRs on the other hand have me scrolling through consultation and progress notes in size 10 text, stacked one on top of each other, which are about as search-able as a Where’s Waldo scene. As a Hospital Medicine doctor who needs to rapidly assimilate information often in the middle of the night – EHR is my last resort. When I receive an emergent page, I rely on my examination, the patient interview (if they’re able to talk), and then a quick glance at a rudimentary ‘sign out’ document handed to me from the day-team. EHR is neither optimized for mobile in most cases, nor can I find anything I am looking for when I actually need it. This is true irrespective of whether I am working at a rural hospital in Maine with a 10 year old EHR, or at a major academic center with a ‘cutting edge’ EHR.
Despite heavy investment in healthcare IT from institutions – providers like myself still find ourselves carrying around printed patient lists with scribbled check boxes and to do lists. The sign out document – a purportedly succinct summary of the patient problems and suggested plan of action quite obviously has pitfalls. One night last week I counted 42 patients I was covering overnight on five different sub-specialty services; and some basic math revealed that in my 12 hour shift I was in charge of more than 120 active medical problems, and at least 1000 years of medical history (conservatively). All of this was summarized for me by other providers in a neatly typed word document extracted from copy-pasted snippets of EHR notes, printed, stapled, and then folded – ready in my white coat pocket for me to peruse while I bolted through corridors or took the elevator to where a patient was crashing.
On discussing the shortfalls of modern healthcare IT solutions; I often hear colleagues stating that change is coming ‘soon’ (read; 2–5 years). Given that medical errors now kill more than 400 000 Americans and are the number three cause of death in the United States – we need a greater sense of urgency about how broken IT systems are, and how we can fix them immediately. Infinitely more thought, investment and energy goes into social networking endeavors than how patient information is presented and made available to healthcare team members. (It is irrefutably easier for me to find out where you went to college – using LinkedIn, Google, or Facebook — than to find out who my patient’s primary care doctor is).
It makes little sense that modern medicine offer us marvels like whole genome sequencing, while simultaneously providing ridiculous solutions such as mnemonics to reduce errors during change of shift. Surely the bar must be set higher, and we must harness the technology we carry in our pockets.
11/4/2014
Varun Verma, M.D. is a board-certified Internal Medicine physician who splits his time as a Hospitalist at Brigham and Women’s Hospital (Boston) and as a Senior Clinical Advisor to Possible (Nepal)
@VarunVermaMD

 RSS Feed
RSS Feed
